Endometrial Hyperplasia
When There Are Signs Of Pre-Cancer
![]()
![]()
Endometrial Hyperplasia |
 |
Endometrial HyperplasiaContents • Endometrial Hyperplasia: Definition |
Return To Main Guide |
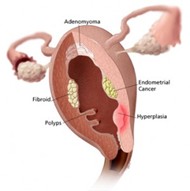
What is Endometrial Hyperplasia?
Endometrial hyperplasia is a thickening in the lining of the womb due to excess cell growth. To be exact, it is defined by an abnormal growth of endometrial and stromal cells which some experts believe is a pre-cancerous condition or precursor to endometrial cancer (uterine/womb cancer). It can occur in women of all ages and can be compared to other pre-cancerous growths like CIN, cervical intraepithelial neoplasia which is linked to cervical cancer. Sometimes the area of hyperplasia (excess cell growth) can return to normal with or without medical treatment. Other times it persists and if left untreated can progress to true cancer. There is no way of telling which will happen. The risk is taken more seriously if 'atypical' or ‘adenomatous’ cells are noted on a pathology report. The development of hyperplasia into cancer, if it occurs, is quite slow, and usually takes 5 years or more. That said, in younger women endometrial hyperplasia is rarely cancerous and in older women it is highly treatable.
The condition is thought to result from an excessive presence of the hormone estrogen. As this hormone imbalance is also linked to cancer of the uterus, it is for this reason that hyperplasia is sometimes considered a precancerous condition. Women who are exposed less regularly to the hormone progesterone are at increased risk of hyperplasia. Progesterone is normally produced after ovulation which is why premenopausal women are less at risk. Women nearing menopause (when ovulation is erratic) or postmenopause women (when ovulation has stopped) are more at risk. Some teenagers, just past menarche who have not yet established a regular pattern of ovulation are also at risk. Endometrial hyperplasia can also occur in women who have used estrogen replacement therapy (ERT) without supplementing it with progestins (artificial progesterone’s). Hyperplasia is also linked to the breast cancer treatment drug tamoxifen. Women who have irregular periods (oligomenorrhea), abnormal heavy periods (menorrhagia) or regular missed periods (amenorrhea) caused by lack of ovulation, PCOS, obesity or hyperandrogenism (an excess of the male hormones) are at risk. All these conditions have been linked to an excess of estrogen in the body.
The most common symptom is vaginal bleeding in a postmenopausal woman. In premenopausal women any abnormal vaginal bleeding such as unusually heavy or prolonged periods or bleeding in between menstrual cycles can sometimes indicate hyperplasia. See also: symptoms of endometrial cancer. If a doctor suspects hyperplasia a full physical examination is carried out. A sample of the uterine cells will need to be taken to send to a lab for testing. This is usually carried out with an endometrial biopsy which can be completed in the doctor's office. During the procedure a flexible tube is inserted into uterus via the vagina. Using suction a small cell sample from the endometrium is removed through the tube. The procedure only takes a few minutes but may cause some light menstrual-like cramping. The lab will be able to distinguish hyperplasia from endometrial cancer and uterine polyps (a condition which causes thickening in one spot rather than throughout the uterus). Sometimes a cell sample can be taken with a dilation and curettage (D&C procedure), which is usually performed in hospital under general anesthesia. This procedure can sometimes also act a cure by removing enough endometrial tissue to stop abnormal bleeding. (See also, diagnosis of endometrial cancer). Types of Endometrial Hyperplasia If hyperplasia is diagnosed, the next step is to determine the type of hyperplasia present. This is important in deciding the best course of treatment for the patient. Hyperplasia types are defined by the amount of irregular sized glands present and an increase in the glands/stroma ratio. There are four types of hyperplasia, each with their own risk for progression to endometrial cancer: Type: Simple Hyperplasia Type: Complex Hyperplasia Type: Simple with Atypical Type: Complex with Atypical What Are The Treatment Options? If hyperplasia is diagnosed it is important to have a full workup because hyperplasia and cancer cells can be present at the same time. The treatment options will vary according to the woman's age and type of hyperplasia present. Teenagers & Younger Women Women with Atypical Hyperplasia Women, who do not ovulate regularly, can reduce the risk of hyperplasia by taking progestin supplements. Those with polycystic ovarian syndrome and hyperandrogenism usually take the birth control pill for this reason. Postmenopausal women who are taking estrogen replacement therapy to counteract the effects of menopause on the body can reduce their risk of both hyperplasia and endometrial cancer by taking progestins for about 12 days every month.
|
| Related Articles on Endometrial Hyperplasia
For more hormone related issues, see the following: • Endometrial Cancer Staging Back to Homepage: Womens Health Advice |
WOMENS HEALTH ADVICE: ABOUT ENDOMETRIAL CANCER |