Endometrial Cancer Treatment
Treating Uterus Cancer
![]()
![]()
Endometrial Cancer Treatment |
 Brachytherapy |
Endometrial Cancer TreatmentContents • How is Endometrial Cancer Treated? |
Back To Main Guidelines |
How Is Endometrial Cancer Treated?
Endometrial cancer, if diagnosed early, is highly treatable and mostly even curable. Fortunately in the majority of cases in America symptoms of endometrial cancer are discovered early. The treatment plan pursued will depend on the stage (how far it has progressed) and the patient’s general health, age and desire for future children. Once all the test results are returned the doctor (oncologist) will recommend a course of treatment. Early stages of endometrial cancer are usually cured with a hysterectomy as well as the removal of both ovaries and the fallopian tubes. More advanced or virulent cancers may require combining surgery with radiation therapy, chemotherapy or hormonal therapy. If you have received a diagnosis of endometrial cancer, take some time to review the treatment options presented and their side effects. If there is something you do not understand, ask your doctor to explain further. You may also want to consult another doctor for a second opinion. In fact some insurance companies require the patient to do so (although less so with routine cancer treatments). Below is a more detailed look at each treatment option.
Surgical Procedure: Hysterectomy This is the standard treatment for endometrial cancer. Early stages of the cancer are usually treated with a hysterectomy combined with a bilateral salpingo-oophorectomy. This involves the removal of the uterus and cervix, along with the ovaries and fallopian tubes. If the procedure is carried out with an incision in the abdomen this is called a simple or total abdominal hysterectomy (TAH). If the uterus is removed through the vagina this is known as a vaginal hysterectomy. In order to stage the cancer, lymph nodes in the pelvis and round the aorta are also usually removed at the same time. If cancer is more advanced and has invaded the cervix and surrounding tissues (parametrium) then a radical hysterectomy is performed. This procedure involves removing not only the uterus but also the tissues next to the uterus and the upper part of the vagina. The normal hospital stay for a hysterectomy is 3 to 7 days and about 5 to 7 days for a radical hysterectomy. Complications do not occur often, if they do, it will be in the form of infection to the wound, excessive bleeding or damage to the urinary or intestinal systems. Removal of the lymph nodes in the pelvis can lead to a build up of fluids in the legs, a condition known as lymphedema (particularly if radiation is also applied). Note: Different methods of surgery are used to perform a hysterectomy, some are more invasive than others. One of the least minimally invasive is called da Vinci surgery. Ask your doctor if you are a candidate for this procedure.
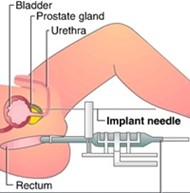
See also: Cancer Surgery Radiation Therapy Options Brachytherapy Radiation may be given externally via a machine or internally by a method called brachytherapy. Vaginal brachytherapy is a procedure sometimes used for gynecologic cancers. It involves placing a cylinder containing a radioactive substance into the vagina. The length of the cylinder can vary. With this method radiation comes into direct contact with the vagina and nearby structures such as the bladder and rectum receives less exposure. This procedure is usually performed about 4 to 6 weeks after a hysterectomy, when the body has had time to heal. There are 2 types of vaginal brachytherapy: Low-Dose Rate (LDR) and High-Dose-Rate (HDR). A LDR device is usually left in place for one to four days and the patient needs to stay in hospital. A HDR is more intense so a device is left in place for less than an hour. The patient can return home the same day. HDR can be given on weekly or even daily basis for at least 3 doses. External Radiation External beam radiation therapy (with a machine) is normally carried out 5 days a week for 4 to 6 weeks. Common side effects of both types of radiation treatment include extreme fatigue, nausea, vomiting and diarrhea - much of which can be controlled by medication. Radiation can cause irritation to the bladder causing what is known as radiation cystitis. It can also lead to low red blood counts and anemia. There may also be some vaginal dryness. Chemotherapy Chemotherapy (or chemo as it is commonly referred as) involves the use of drugs which are taken orally or injected to fight cancer which has spread beyond its original source. In the case of endometrial cancer it may be considered an option where cancer has spread beyond the endometrium (stage 3 and 4, see endometrial cancer staging). The National Cancer Institute and other research groups are studying the benefits of combining surgery with chemo in these instances. The chemo drugs used in trials to date include cisplatin, ifosfamide and doxorubicin. See Chemotherapy guide. This is the use of hormones or hormone blocking drugs to prevent the growth of cancer. This type of therapy is not the same as that given to women to prevent menopause symptoms (i.e. HRT). In the case of endometrial cancer, hormone therapy is commonly prescribed as a way to manage advanced stages of the disease or as an alternative for women who are not strong enough to cope with more aggressive therapies like radiation or surgery. Progestins Tamoxifen GNRH Aromatase Inhibitors
|
| Related Articles on Endometrial Cancer Treatment
For more cancer related issues, see the following: • Endometrial Cancer Survival Rates Back to Homepage: Womens Health Advice |
WOMENS HEALTH ADVICE: ABOUT ENDOMETRIAL CANCER |